
EEn should restock by 05/05/2024, ideally. EC by 19/05/2024.
AN IMMEDIATE RECALL OF ALL TRANSDERMAL GEL PURCHASED SINCE THE END OF AUGUST IS IN EFFECT. YOU ARE ADVISED TO DISCONTINUE USE. IF YOU WERE AFFECTED, YOU WILL HAVE BEEN CONTACTED BY THE EMAIL YOU USED TO PURCHASE FROM US. VIEW OUR INCIDENT REPORT HERE.
Site has moved here, potentially temporarily. Canary has been updated.


Estradiol Undecylate has one of the longest-acting effects of any Estradiol ester, allowing for more stable levels and a greater duration between injections. At 34mg/31 days (0.85ml), a single vial should last a year.
Due to the large volume of this injection required to achieve monthly injections, we recommend intramuscular injection only for this ester. Furthermore, given variations in individual metabolism of esters, combined with the long duration and large volume of this product, we highly recommend obtaining blood tests to more favourably tailor your dosage.
Unlike other half-life curves, the exact half life of Estradiol Undecylate included in the attached graph is not representative of data solely from Estradiol Undecylate itself, but is modelled on the half-life curves of Testosterone Undecylate (which has a similar fat solubility to Estradiol Undecylate) and informed by case reports and studies on Estradiol Undecylate. The precise average levels should be similar to the given graphical representation, but minor variation should be expected. The reason for this is that Estradiol Undecylate was only offered by a limited number of pharmaceutical companies before it was ultimately discontinued several decades ago. Because of this, there is limited modern data on the precise elimination curves of Estradiol Undecylate, and older data (often half a century old or more) is of poor quality. For more information on this and the simulator from which these curves originate, please see here.
Store in a cool, dry place, out of direct sunlight. Not suitable for refrigeration.
If vial stopper becomes compromised, or changes occur in visual clarity or viscosity of oil solution, discard. If vial coring occurs, discard.
Recommended reading/viewing at the bottom of the page if this is your first time using injections.
All recommended dosages are suggestions for monotherapy only, pre-orchiectomy, and should be informed and adjusted based on bloodwork. For bloodwork, Estradiol levels should be taken at trough, up to 24 hours before your next dose. Target trough levels should be roughly 200 pg/ml (734 pmol/l) without an antiandrogen, or 100 pg/ml (367 pmol/l) with an antiandrogen in sufficient dosage to suppress testosterone production by the testes. The recommended dosage (34mg/30 days) will likely give you levels easily above these ranges, except for rare individuals who metabolise the Estradiol ester abnormally quickly, if you are able to access bloodwork, it is recommended to adapt your dosage according to target trough levels, either by altering the dosage, or by altering injection frequency.
Estradiol monotherapy is not recommended to cisgender women with intact endometrial tissue as a form of menopause relief or birth control due to risks of cancer and endometrial hyperplasia.
For harm reduction purposes it should be noted that the recommended dosages are only appropriate for adults, and not for children or individuals in their early teens, for whom dosages should be lower.
Most trans individuals, particularly in cold and light deprived regions are deficient in Vitamin D. It is recommended to take supplements to account for this, or spend time outside touching grass during daylight hours.
Vials are theoretically stable for 8+ years, assuming no major alterations in appearance of oil solution. It is not, however, advisable to keep so many on hand, in most cases, and we would recommend no more than 3 vials maximum per individual.
In case of refrigerating at a stable temperature for long term storage, or storing in a cold place, dissolved estradiol might crash out of solution. This will appear as small white crystal dust forming on the bottom of the vial which will lift from the base of the vial when tilted sufficiently to displace it where it will stick close together in a thin ribbon of crystalline white dust suspended in oil near the bottom of the vial. To return it to solution, warm the vial in hot water and shake thoroughly.
Out of stock
| Ingredients | Estradiol Undecylate (400mg), MCT Oil (53.9%), Benzyl Benzoate (44.1%), Benzyl Alcohol (2.0%) — All percentages by weight |
|---|---|
| Concentration | 40mg/ml |
| Total Volume | 10ml |
| Total Active Ingredient | 400mg |
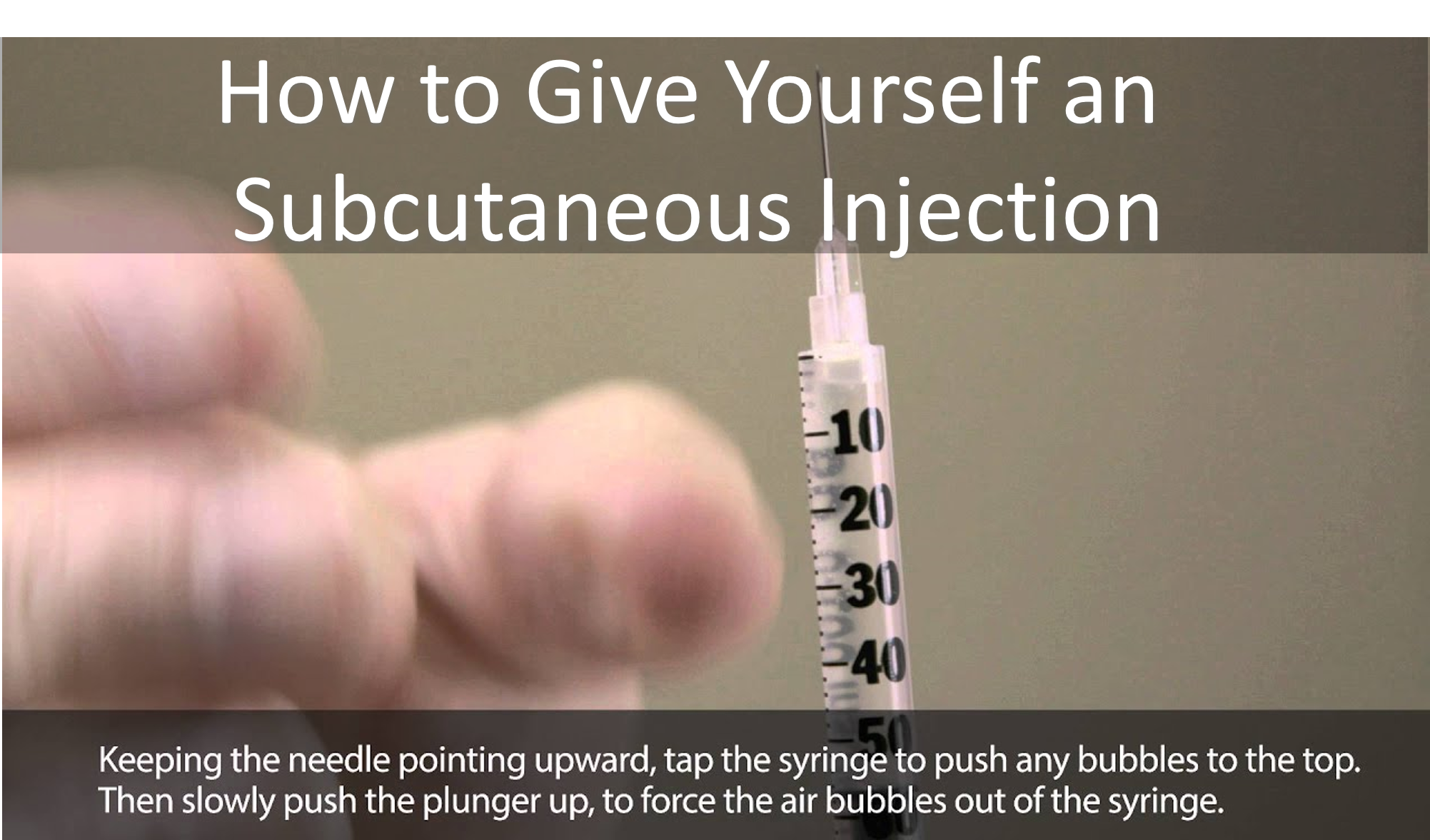
| Final Notes | If vial stopper becomes compromised, or changes occur in visual clarity or viscosity of oil solution, discard. If vial coring occurs, discard. Redness or irritation post-injection may be a result of localised irritation, improper aseptic technique, contamination of the vial, Benzyl Alcohol or Benzyl Benzoate—a solvent used too facilitate the dissolving of the Estradiol ester contained within this vial. While not currently available, variations with lower/absent concentrations of Benzyl Benzoate will be available at a later date, compounded in a different Carrier Oil. Always follow proper disinfection technique and ensure proper storage and examination of vials prior to use. Ensure no large air bubbles remain in your syringe during injection. If you have congenital heart issues or a family history of breast cancer, consult a doctor. Anecdotal observation suggests that severe connective tissue disorders are more common in trans individuals. If you are hypermobile with a history of joint pain, subluxation, dislocations, or unexplained weakness of cardiac valves, please consider the following: |
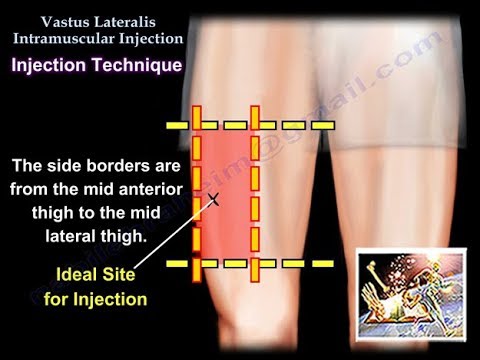
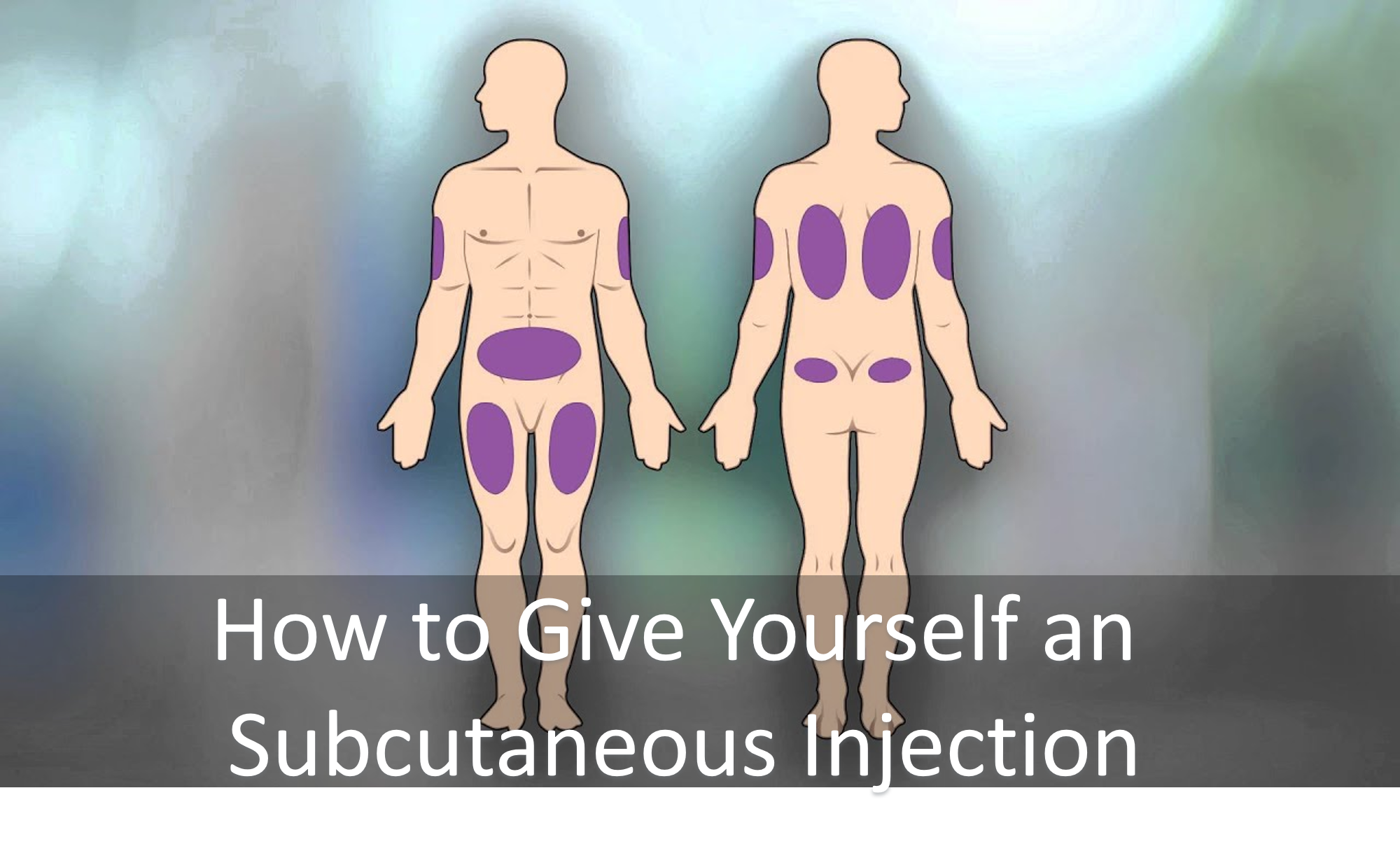
We recommend the vastus lateralis (thigh) injection site for beginners to self-injection. Please note that subcutaneous and intramuscular injection sites might not coincide with each other. Find the sites appropriate for your method of administration. Subcutaneous injection might lead to minor irritation or redness, intramuscular injection can reduce or resolve that.
Select only sterile, individually wrapped needles and syringes. If using a sterile, individually wrapped filter unit or filter needle (not a Frontier Medical Filter Needle which is not applicable for vials), only use the filter for either drawing or injecting. This will require replacing the needle unit placed on the tapered top of the syringe after drawing from the vial.
When selecting needle sizes, the size is represented by gauge. Larger needle diameters(represented by a smaller gauge number – 18G vs 29G) can lead to greater pain at the injection site if used. However, given the viscosity of oil injections, be aware that needles with smaller diameters (larger gauge, e.g. 29G) take longer to fill. Individuals with higher body fat may require longer needles for intramuscular injection. Finally, be aware that insulin syringes show “insulin units” not millilitres. Each 10 units is equivalent to 0.1ml. Please keep this in mind when using insulin syringes.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Reviews
There are no reviews yet.