
EEn should restock by 05/05/2024, ideally. EC by 19/05/2024.
AN IMMEDIATE RECALL OF ALL TRANSDERMAL GEL PURCHASED SINCE THE END OF AUGUST IS IN EFFECT. YOU ARE ADVISED TO DISCONTINUE USE. IF YOU WERE AFFECTED, YOU WILL HAVE BEEN CONTACTED BY THE EMAIL YOU USED TO PURCHASE FROM US. VIEW OUR INCIDENT REPORT HERE.
Site has moved here, potentially temporarily. Canary has been updated.
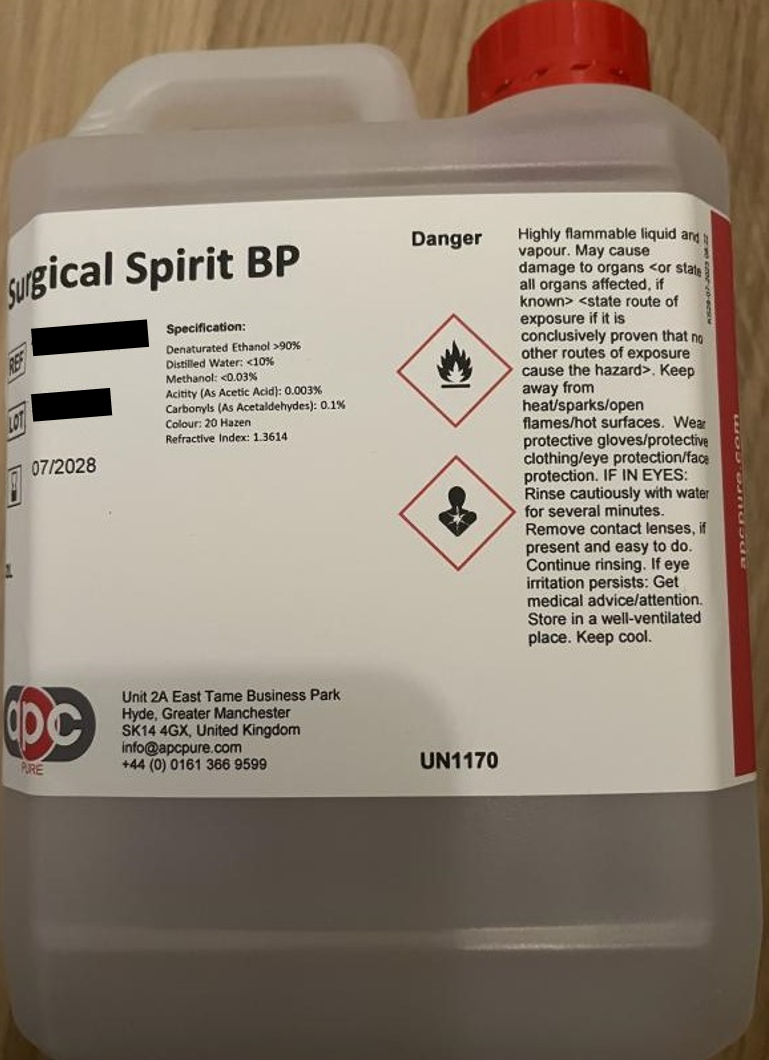
Recently, we were contacted concerning the inclusion of methanol within our gel. Methanol is a common alcohol denaturant used within the UK. It is a by-product of ethanol synthesis and exists as an impurity. 5% (v/v) methanol is combined with 95% (v/v) ethanol in the UK to make “industrial methylated spirit”, which is then used in Surgical Spirit BP which is used as a topically applied skin cleanser and antiseptic (see here and here), and can be legally sold for topical cutaneous use within the UK (see here) since the main risk of methanol poisoning is from oral consumption.
Industrial methylated spirit is the former name of what is now known as Industrial Denatured alcohol (see here), it is approved in the UK for external medical applications (see here (10.1.2), here, and here).
After supply issues, following which, the original TSDA we used was no longer available we switched to a Surgical Spirit BP from a large chemical supplier that was advertised for topical use at the end of August 2023. Surgical Spirit BP is a legal classification requiring certain standards for its production.
After purchase we instead received something that misrepresented itself as Surgical Spirit BP, and was labelled as such, but lacked the legally required formulation by the British National Formulary/British Pharmacopoeia.
Following our end of August restock, we updated the website with the details on the container, relying on the legal requirements for minimum standards laid out by the BNF and BP to hold. In hindsight, this was clearly a grave error.
We once again updated our site late last month while restoring from a backup following a DDoS attack which resulted in being dropped by our hosts.
However, we only realized we’d been sent something claiming to be Surgical Spirit following a contact about the methanol content within our gel. This methanol content was acceptable within legal standards laid out for cutaneous medical use by HMRC, BP, and BNF.
Denatured Ethanol: >90%
Distilled Water: <10%
Methanol: <0.03%
Acidity (As Acetic Acid): 0.003%
Carbonyls (As Acetaldehydes): 0.1%.
However, as a result of this contact we set to examining the constituents more closely, we later found that one of the excipients was acetaldehyde, though it was not the subject of the questioner’s concern.
By fortune rather than any particular foresight, the overall final concentration of acetaldehyde in the gel appears to be low enough and theoretically incapable of sufficient transdermal absorption to cause any significant toxicity, but this is no excuse. Acetaldehyde is classed as a Class 2B Carcinogen by the IARC meaning that there is the possibility that it can cause cancer. This is the second lowest risk class of IARC designated carcinogen (with Class 3 being “Not classifiable as to its carcinogenicity to humans”) and it includes things like Nickel, Pickled Vegetables, and Progestins. You can get a more in depth idea of what the classifications mean here, but the quick explanation is that for Class 2B a certain quantity of the named substances shows either limited or inadequate evidence of carcinogenicity in humans.
The limitations on use of acetaldehyde in topical applications is generally considered to be one of lacking long term data on chronic dermal exposure, though theoretical extrapolations of current evidence indicate a low transdermal absorption, lacking in carcinogenicity by the dermal route. This has, in the past, resulted in recommendations of extreme caution regarding dosing of acetaldehyde in topical applications, and thus the use of worst case scenario estimates of safe exposure levels using 100% absorption. Fortunately, however, more recent studies than past committee rulings on safety seem to indicate that this assumed 100% absorption rate is not the case.
As we will be going over in the following write up, the only carcinogenic effects to have ever been identified from acetaldehyde exposure are in airway mucosal tissues as a result of chronic inhalation of extremely high atmospheric concentrations of acetaldehyde (industrial accident levels). You will not have experienced anywhere close to these atmospheric concentrations for even a short period of time and the possibility of achieving these atmospheric concentrations through normal use of gel even for a fraction of a second are close to nil.
Likewise, exposure levels to acetaldehyde in the gel (assuming 100% absorption) are less by two orders of magnitude than exposure levels to acetaldehyde seen in the course of average daily dietary nutritional intake.
Regardless of fraud and willful misrepresentation by the supplier, we are ultimately responsible and the buck stops with us. We have failed you; for that we are deeply regretful and ashamed. We deserve any rightful anger you might be feeling. We are sorry.
65.1% Ethanol (here: Surgical Spirit) is used in 1000 grams of gel solution, to create 1123.6ml of gel at 25°C
This means 1 kilogram of gel contains at most
0.0003 x 650.667 grams of methanol = 0.1952 grams of methanol
0.001 x 650.667 grams of acetaldehyde = 0.6507 grams of acetaldehyde
Since 1 kilogram of gel is 1123.6 millilitres, 1 litre contains at most
0.1952 ÷ 1.1236 = 0.1737 grams of methanol
0.6507 ÷ 1.1236 = 0.5791 grams of acetaldehyde
1 millilitre of gel therefore contains at most
0.1737 ÷ 1000 = 0.0001737 grams = 0.1737 milligrams of methanol
0.5791 ÷ 1000 = 0.0005791 grams = 0.5791 milligrams of acetaldehyde
0.2 millitres of gel (1 pump) contains at most
0.1737 x 0.2 = 0.035 milligrams of methanol
0.5791 x 0.2 = 0.116 milligrams of acetaldehyde
0.8 millitres of gel (4 pumps) contains at most
0.1737 x 0.8 = 0.139 milligrams of methanol
0.5791 x 0.8 = 0.463 milligrams of acetaldehyde
The levels of methanol within the gel, are safe both for the safe reference dose of 0.5 mg and the more recently revised reference dose of 2.0 mg/kg body weight per day[[1]] supplementary to a normal dietary intake. This is even assuming 100% absorption, which is highly unlikely. Additionally, average methanol consumption is estimated at 1,000 mg per day, owing mostly to vegetables and fruit [[2]].
However, the alleged surgical spirit showed it also contained acetaldehyde, which is a byproduct of fermentation, and present in many foods, including fruit, fruit juices, vegetables, bread, and alcoholic beverages. It is also used as a flavour additive in soft drinks and sweets.
Furthermore, ethanol is broken down into acetaldehyde in the liver as an intermediate step of alcohol metabolism. The rate of alcohol metabolism in humans is roughly 170 to 240 g per day, 7-10 g per hour, and 116-167 mg per minute in 70kg individuals though there is wide variation in individual tolerance [[3]]. Given that some individuals can consume 200-300 g of alcohol in a day, this can cause serious metabolic stress, and also production of acetaldehyde [[3]]. The average exposure to acetaldehyde in alcoholic beverages is thought to be 0.112 mg/kg body weight per day [[4]], or 7.84 mg for an individual weighing 70kg (not including acetaldehyde that is an intermediate product of alcohol metabolism).
Acetaldehyde is classified as a Class 2B carcinogen [[5]] meaning that it is “Possibly carcinogenic to humans” [[6]], this is the classification for substances with limited or inadequate evidentiary basis of carcinogenicity in humans; however, when “associated with consumption of alcoholic beverages” acetaldehyde is classified as a Class 1 carcinogen [[5]] meaning that it is “Carcinogenic to humans” [[6]]. The 4 classifications from the IARC is as follows.
| Group 1 | Carcinogenic to humans | 127 agents |
| Group 2A | Probably carcinogenic to humans | 95 agents |
| Group 2B | Possibly carcinogenic to humans | 323 agents |
| Group 3 | Not classifiable as to its carcinogenicity to humans | 500 agents |
Other examples of Class 2B carcinogens include: Aloe Vera extract, Catechol (an molecule that naturally occurs in fruit and turns reddish brown when oxidised, resulting in the bruising of fruit), Phenytoin (an anti-epilepsy medication), Nickel, Pickled vegetables, Progestins, and Carpentry and joinery [[5]].
The Joint FAO/WHO expert committee estimated daily intake of acetaldehyde as a flavour additive at 9.7–11.0 mg per day [[7]]. The Japanese FSC estimated daily intake as a flavour additive at 9.618–19.211 mg[[8]] and cited the work of Stofberg J. & Grundschober F. [[9]] to estimate intake of natural dietary intake to be fourfold that used for flavouring, for a total exposure of 48–96 mg/day [[8]]. FEMA places average dietary intake at 35.261 mg/day [[10]], Morris et al. reiterates FEMA’s estimate at 35 mg/day and presents an example diet that yields 75 mg/day, while also citing the worst case dietary levels of 200 mg/day put forward by Technical Assessment Systems (TAS)[[11]].
While understandably concerning, it is also worth noting that the equivalent amount of acetaldehyde in 0.8 ml, or 4 pumps, of gel (0.463 milligrams) is equivalent to that directly present in: a half kilo of apples; 81 grams of apple juice; 120 grams of orange juice; 26.5–167 grams of yoghurt (depending on the yoghurt); 103 grams of canned peas; 309 grams of wheat and rye bread; 12 grams of certain roasted coffee powders (about 1 cup of coffee) [[12]]; 31-463 ml of beer (1/20th – 4/5th of a pint) [[13]]; 5–9 ml of wine [[14]]; 1–5ml of sherry wine [[15]]; and under 6% of the average 70kg individual’s direct daily consumption of acetaldehyde contained in alcoholic drinks (before alcohol metabolism) [[12]].
All of the above are for oral use, unlike gel, and the majority of gel use will likely be under 0.8 ml. Nor would gel meet the criteria of a Class 1 Carcinogen since it’s not associated with alcohol consumption.
Any ethanol or acetaldehyde would therefore be absorbed through the skin or inhaled from evaporation.
Transdermal absorption of ethanol in ethanol based hand sanitizer is negligible or nil in cases of regular use [[16]]. Even in excessive application, transdermal absorption is minimal. The even application of 80 millilitres of ethanol hand sanitizer (55%) over a 30 minute period showed absorption at a rate of only 0.9% [[17]].
A study by Thredgold L. et al showed transdermal absorption (the measure of a chemical’s ability to pass through the upper layers of the skin and travel into the body) of acetaldehyde is low even in cases of full body exposure at 996 ppm. Over a 30 minute timespan, average absorption was 22 µg/cm2 [[18]]. In this study, the atmosphere was filled with 996 ppm acetaldehyde for 30 minutes yielding 22 micrograms (or 0.022 milligrams) of dermal absorption over this time. Dermal absorption was 9 micrograms (or 0.009 milligrams) per cm2 at 20 minutes constant exposure [[18] [figure 2.]]. Dermal absorption was approximately 1 microgram ( or 0.001 milligram) per cm2 at 10 minutes constant exposure [[18] [figure 2.]]. We can see from this that acetaldehyde is absorbed roughly linearly with time.
Dermal penetration (the measure of a chemical’s ability to enter and remain in the upper surface of the skin, the stratum corneum – taken using tape/swabs to find the presence of a chemical in the upper dead layers of skin) in the same study also showed an average dermal penetration of 5.29 µg/cm2 at 30 minutes continuous exposure, an average dermal penetration of approximately 3.40 µg/cm2 at 20 minutes continuous exposure, and an average dermal penetration of approximately 0.80 µg/cm2 at 10 minutes continuous exposure[[18] [figure 1.]]. Once again this seems to show that acetaldehyde penetrates the skin roughly linearly with time.
Morris et al. stresses the importance of route specific carcinogenicity, noting that inhaled acetaldehyde is 14–35 times less potent on nasal mucosa than equal doses of inhaled formaldehyde, and 5 times less potent in terms of gastric injury when ingested, furthermore noting that the stomach is 10–60 times less sensitive to acetaldehyde and formaldehyde than the nasal mucosa. He goes on to note that while causing injury, such as stomach lesions, orally ingested formaldehyde lacks the carcinogenicity in the stomach that it displays in the nasal mucosa, and uses the pattern of reduced sensitivity to extrapolate a similar lack of tumorigenicity for orally ingested acetaldehyde—though he does note the importance of long term studies over simple extrapolation, despite its utility [[11]], though such studies are often confounded by other environmental and behavioural factors. Acetaldehyde’s decreased sensitivity relative to formaldehyde would indeed fit with its profile shown in the transdermal absorption study by Thredgold L. et al, where acetaldehyde’s power to cross barriers such as the epidermis and enter non-superficial cutaneous tissues is severely limited compared to that of formaldehyde [[18] [figure 2.]].
Corollary to this, the ECHA noted that no convincing evidence of formaldehyde dermal carcinogenicity existed, expressing that only the route of inhalation demonstrated tumorigenic effects, and even then only at doses sufficient to produce chronic irritation [[19]]. Animal studies on dermal application of formaldehyde likewise showed no carcinogenic effect, though when combined with another strong carcinogen while it didn’t increase the overall number of tumors formed, it did accelerate the speed at which they first appeared and the mean latency of carcinogenesis [[20]]. Given the decreased sensitivity of tissues compared to formaldehyde, and the relationship between acetaldehyde and formaldehyde sensitisation, it seems reasonable to extrapolate an equally low or lower dermal carcinogenicity for acetaldehyde. Where, for formaldehyde, the ECHA noted “Overall, there is no convincing evidence of a carcinogenic effect at distant sites or via routes of exposure other than inhalation” [[19]].
Following on ECHA’s note of carcinogenicity only occurring at doses sufficient to produce chronic irritation, it is possible that outside of inhalation, acetaldehyde’s mechanism of carcinogenesis when associated with alcoholic beverage consumption stated by IARC [[5]] is due to irritant levels of acetaldehyde associated with the nutritional and metabolic acetaldehyde burden associated with alcoholism, whereas regular dietary intake fails to produce irritation.
With an upper bound dosage of 0.8 millilitres of gel, only 0.463 milligrams of acetaldehyde would ever typically be dispensed. If all of this evaporated into the air, and remained in a 1m3 area at all times, this would only be equivalent to 0.463 mg/m3. Furthermore, with a molecular weight of 44.05 g/mol, we can calculate the ppm concentration of the contained quantity of acetaldehyde with the following formula:
Concentration (ppm) = 24.45 x concentration (mg/m3) ÷ molecular weight
24.45 x 0.463 mg/m3 ÷ 44.05 g/mol = 0.2569
https://www.cdc.gov/niosh/docs/2004-101/calc.html
Here we can see that the given atmospheric concentration would be 0.257 ppm (or 257 ppb), meaning any evaporated acetaldehyde poses negligible inhalation risk at over 3,800 times smaller than the concentration in the above transdermal absorption study by Thredgold L. et al. (the concentration (mg/m3) of this study works out to 1794.429 mg/m3), assuming that 100% evaporates and remains within one cubic meter. In reality, acetaldehyde that evaporates will disperse to irrelevance exceedingly quickly.
Comparing the 22 µg/cm2 average absorption of 1794.429 mg/m3 for 30 minutes to that of 1 µg/cm2 for 10 minutes, any dermal absorption through evaporated acetaldehyde would be extremely surprising.
However, were it to circulate around an individual, constantly replenishing itself for the next two years, it would still be 194 times lower than what would be required to produce any irritation in the human eye, 583 times lower than what would produce nose or throat irritation in humans [[21]] which are some of the most sensitive tissues to irritants in the human body. Furthermore it would be far below almost, if not all, existing safety guidelines on acceptable atmospheric concentrations for long term workplace exposure.
The majority of applied gel should evaporate within 15-20 seconds. This is 90-120 times shorter in duration of exposure to the concentrated atmosphere of Thredgold L. et al. It is over 1400 times shorter than the long term workplace exposure guidelines, most of which are for given durations of 8 hours.
Compounding to this rapid evaporation time, the boiling point of acetaldehyde is 20.2°C, compared to ethanol at 78.4°C, which will result in its extremely rapid evaporation upon skin contact and further reducing the potential for exposure and absorption.
With 22 µg/cm2 average absorption of 1794.429 mg/m3 for 30 minutes, it is readily apparent that 0.463 mg/m3 for a dozen seconds at most will be of negligible effect. Even more so when considering the 1 µg/cm2 average absorption for a duration of 10 minutes. There is simply insufficient time for absorption compared to its boiling point and the atmospheric concentration the gel can produce is insufficient to generate the required high concentrations seen in the study by Thredgold L. et al.
Penultimately, reinforcing the superior absorption of the oral route, as expected using Morris et al.’s extrapolation: while the oral toxicity of acetaldehyde is assessed at 1,230 mg/kg of bodyweight [[22]], the dermal toxicity requires dosages almost fourfold higher, once again pointing toward the poor dermal absorption of acetaldehyde. The SCCS stated the following about the acute dermal toxicity of acetaldehyde:
“By the dermal route of exposure Acetaldehyde is practically non-toxic. A dermal LD50 value of greater than 5,000 mg/kg bw has been reported in rabbits on the basis of single death in 10 animals administered 5,000 mg/kg bw” [[23]]
Finally, IMAP concluded that acetaldehyde was not a skin irritant, though they did note that some studies with high concentrations of acetaldehyde did produce slight irritation, and that patch tests in human volunteers resulted in erythema at 10% formulations, adding that concurrent exposure to other chemicals in the preparation might have contributed to the resultant irritation [[24]].
The low quantities of acetaldehyde present in a typical dosage of gel are insufficient to produce irritant responses upon inhalation, nor are they sufficiently sustained to generate the chronic irritation that is a prerequisite for carcinogenicity seen with the far more potent formaldehyde.
The oral route is not applicable to the usage of gel, but incidental exposure to the oral pathway will have negligible impact due to only trace amounts of acetaldehyde and ethanol being consumed.
On the basis of acetaldehyde’s low boiling point, and thus rapid evaporation, it is unlikely to have time to achieve transdermal absorption. This lack of ability to easily cross into bodily tissues in meaningful quantities is reinforced by the small area of application, the lack of dermal irritation upon exposure, the incredibly low dermal toxicity compared even to oral application, and the vast difference in transdermal absorption between formaldehyde and acetaldehyde.
Furthermore, given the lack of convincing evidence of carcinogenic effect of formaldehyde upon dermal exposure, the likelihood of a less potent, less readily absorbed substance such as acetaldehyde having significant carcinogenic effects where formaldehyde failed is low. Likewise, the comparatively high daily oral intake of acetaldehyde as part of a natural diet, and the rapid metabolism of acetaldehyde compared to the quantities present in a daily dose of gel would make dermal carcinogenicity extremely surprising. Low transdermal absorption of ethanol should likewise reduce simultaneous exposure to large amounts of ethanol.
Given that transdermal absorption should be limited, and any carcinogenicity unlikely to result from it, we consider the realistic risk of toxicity resulting from acetaldehyde exposure occurring during normal use of the gel to be negligible.
Regardless, continued usage of affected gel is still discouraged.
A request for information on the methanol content of our gel was received. Concentration of methanol within the gel was deemed to be well within safe reference guidelines for daily application.
Though not included in the request, it also brought to our attention the acetaldehyde content of the gel, which was part of the alleged surgical spirit. The acetaldehyde content per dose of gel is far below the average daily exposure from a regular diet.
The alleged surgical spirit will be immediately disposed of.
The supplier will no longer be utilised for purchases of any materials.
Oral absorption was deemed to be non applicable to route of administration.
Low resultant atmospheric concentrations of acetaldehyde from evaporation preclude significant absorption through inhalation and resultant carcinogenicity.
Insufficient long term studies on dermal toxicity of acetaldehyde exist to know the exact toxicity. The absorption of acetaldehyde through the skin is believed safe at given quantities, due to low content of acetaldehyde per dose, acetaldehyde’s low boiling point and difficulty in crossing the surface barrier of the skin. Continued usage is still discouraged
New processes will be put in place to pursue further verification of ingredients.
Gel will be reformulated using either isopropyl alcohol or, preferentially, suitable ethanol, if available. We’re aiming for a fast turnaround time on this to limit delays and waits associated with this.
All affected gel will be immediately recalled and orders refunded.
Affected individuals may also, if they wish, in addition to the refund, receive replacement reformulated gel, once produced.
If you have been affected by this, or are unsure if you have been affected by this, email us with “Recall” included in your message title.
[1] EPA — Integrated Risk Information System (IRIS) Methanol — https://iris.epa.gov/static/pdfs/0305_summary.pdf
[2] COMMITTEE ON TOXICITY — COT STATEMENT ON THE EFFECTS OF CHRONIC DIETARY EXPOSURE TO METHANOL — https://cot.food.gov.uk/sites/default/files/cot/cotstatementmethanol201102revjuly.pdf
[3] Cederbaum A — ALCOHOL METABOLISM — https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3484320
[4] Lachenmeier DW et al. — Carcinogenicity of acetaldehyde in alcoholic beverages: risk assessment outside ethanol metabolism — https://pubmed.ncbi.nlm.nih.gov/19335652/ (sci-hub link)
[5] IARC— List of Classifications — https://monographs.iarc.who.int/list-of-classifications
[6] IARC — Agents Classified by the IARC — https://monographs.iarc.who.int/agents-classified-by-the-iarc
[7] JECFA — SAFETY EVALUATION OF CERTAIN FOOD ADDITIVES AND CONTAMINANTS — https://inchem.org/documents/jecfa/jecmono/v040je10.htm
[8] FSC — Evaluation Report of Food Additives Acetaldehyde — https://www.fsc.go.jp/english/evaluationreports/foodadditive/acetaldehyde_report.pdf
[9] Stofberg J, Grundschober F — Consumption Ratio and Food Predominance of Flavoring Materials — https://img.perfumerflavorist.com/files/base/allured/all/document/2009/10/pf.PF_12_87_027_32.pdf
[10] Burdock GA — Fenaroli’s Handbook of Flavour Ingredients – http://www.t27.ir/Files/121/Library/df16c9a2-21d3-46b2-b0b3-e543193278b4.pdf
[11]Morris et al. — A Parallelogram Approach for Safety Evaluation of Ingested Acetaldehyde — https://www.sciencedirect.com/science/article/abs/pii/S0273230096901385 (sci-hub link)
[12] Uebelacker M, Lachenmeier DW — Quantitative Determination of Acetaldehyde in Foods Using Automated Digestion with Simulated Gastric Fluid Followed by Headspace Gas Chromatography — https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3124883
[13] Brewers Association— BEER OFF FLAVOR: Acetaldehyde — https://cdn.brewersassociation.org/wp-content/uploads/2021/07/22092751/Beer_Off_Flavor_Acetaldehyde.pdf
[14] IARC — Chemical Composition of Alcoholic Beverages, Additives and Contaminants — https://www.ncbi.nlm.nih.gov/books/NBK531662/
[15] Garcia L et al. — Impact of Acetaldehyde Addition on the Sensory Perception of Syrah Red Wines — https://www.mdpi.com/2304-8158/11/12/1693
[16] Brewer C, Streel E — Is Alcohol in Hand Sanitizers Absorbed Through the Skin or Lungs? Implications for Disulfiram Treatment — https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7454269
[17] Kramer A. et al.— Quantity of ethanol absorption after excessive hand disinfection using three commercially available hand rubs is minimal and below toxic levels for humans — https://bmcinfectdis.biomedcentral.com/articles/10.1186/1471-2334-7-117
[18] Thredgold L. et al.— Understanding skin absorption of common aldehyde vapours from exposure during hazardous material incidents — https://www.nature.com/articles/s41370-019-0127-4 (sci-hub link)
[19] ECHA RAC — Opinion proposing harmonised classification and labelling at EU level of Formaldehyde — https://echa.europa.eu/documents/10162/b8dfa022-9544-72e8-dcaa-7491dff3c0d5
[20] Iversen O.H. — Formaldehyde and skin carcinogenesis — https://www.sciencedirect.com/science/article/abs/pii/0160412086901480 (sci-hub link)
[21] Emergency and Continuous Exposure Guidance Levels for Selected Submarine Contaminants: Volume 3 — https://www.ncbi.nlm.nih.gov/books/NBK219914
[22] Drinking Water and Health: Volume 1 — https://pubmed.ncbi.nlm.nih.gov/25032358/
[23] OPINION OF THE SCIENTIFIC COMMITTEE ON COSMETIC PRODUCTS AND NON-FOOD PRODUCTS INTENDED FOR CONSUMERS — https://ec.europa.eu/health/archive/ph_risk/committees/sccp/documents/out275_en.pdf
[24] IMAP — Acetaldehyde: Human health tier II assessment
—https://www.industrialchemicals.gov.au/sites/default/files/Acetaldehyde_Human%20health%20tier%20II%20assessment.pdf